
In non-extraction orthodontics, we avoid extracting healthy bicuspid teeth to make space.
(From Wikipedia: The premolar teeth, or bicuspids, are transitional teeth located between the canine and molar teeth. In humans, there are two premolars per quadrant in the permanent set of teeth, making eight premolars total in the mouth. They have at least two cusps.)
This can be easily accomplished by early intervention therapy and jaw orthopedics. Special consideration is given to achieving and promoting an enlarged airway, a healthy jaw joint, a fully developed, wide smile, and a pleasing facial profile with proper lip support.
The guiding principle “First do no harm!” implies that extracting perfectly healthy teeth in order to ‘create space’ in a jaw that is not big enough to accommodate all teeth, is a biological mistake. If jaw orthopedics is initiated precisely when the jaws are still developing (ages 5-11), this notion becomes obsolete. The trick is to MAKE space early, not to amputate healthy teeth later.
 Take, as an example, the series of images: This little girl started out with a lower jaw that was too small. This might have been considered cute at this age, but as a young adult, that smaller jaw would have taken away from a pleasing profile. The latest development (bottom image) shows her after a very successful early intervention jaw orthopedics appliance therapy – this is a girl who will – growing up – exhibit facial harmony, a beautiful profile, self-esteem, and determination, that would never be possible with an underdeveloped chin.
Take, as an example, the series of images: This little girl started out with a lower jaw that was too small. This might have been considered cute at this age, but as a young adult, that smaller jaw would have taken away from a pleasing profile. The latest development (bottom image) shows her after a very successful early intervention jaw orthopedics appliance therapy – this is a girl who will – growing up – exhibit facial harmony, a beautiful profile, self-esteem, and determination, that would never be possible with an underdeveloped chin.
Principles
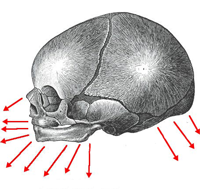
There are growth centers in the jawbones that direct jaw growth in three fundamental dimensions: a slightly downward direction, responsible for vertical development of the jaws; a forward direction to help develop a pleasing profile; and a horizontal direction which aids lateral development.
Our genes determine the functioning of those growth centers. If any of those developments are disturbed, we can aid the jaw development with movable or fixed appliances to nudge those growth centers.
Read more in Principles of Functional Jaw Orthopedics…
What are early signs of crowding?
There are multiple signs of impending insufficient jaw size and crowding that parents and physicians need to watch out for in children. Identifying these is a key factor in seeking early jaw orthopedic therapy. This may change your child’s life.
Following are signs of future crowding:
- front crossbite (provide links to each section – originally in FAQ section, however move each of these to a separate article in the articles section which will also allow me to expand the section)
- Side crossbite
- No Space For Lateral Incisors
- Flared lateral incisors
- Displaced canines
- Overclosed bite
Strategies
The first signs that the jaw development of a child is not progressing optimally are crowded teeth, a crossbite, or similar manifestations. Traditionally braces were used, possibly after extracting perfectly good teeth to create space, to handle the situation.

Now we understand that these signs are just symptoms and that we must first handle the underlying dysfunction. This is done with early intervention during the maximum growth phase of a child during the ages of 5 (6) to 10 (latest 11).
At age 10 we might have missed the early jaw orthopedics phase, as eighty percent of jaw growth has already occurred. During this time most of the primary teeth are either loose or already lost, which makes the application of removable appliances very difficult. If this early phase is missed, braces will probably take longer.
To gain a deeper understanding of the strategies employed in early intervention and to understand the positive health effects on opening the airways, lip closure training, and nose breathing, read the pages on Strategies of Functional Jaw Orthopedics…