There are many signs of early malocclusion, future crowding, childhood sleep apnea or skeletal growth discrepancies that parents should be aware of. Some of these conditions have to be addressed immediately, and others in due time before the child exits the rapid growth phase. Most signs go hand in hand with arch and jaw underdevelopment. Many of these signs are ignored or just not detected by most general dentists and physicians, but it is imperative that they are identified while the child is still within the growth phase, a window of opportunity that presents itself only once in a lifetime.
DENTAL SIGNS:
(these usually require early intervention arch development)
- SPACES BETWEEN BABY TEETH: If there are no SPACES between the baby teeth, this is a sure indication that there will be crowding in the permanent dentition. Arch development should commence between ages 6-9.

A healthy jaw with healthy tooth spacing 
No spaces between baby teeth will result in future crowding - FRONT CROSSBITE – involving the front teeth: if the lower teeth are biting in front of the upper teeth, it is a situation that demands immediate intervention. The condition will trap the upper jaw from growing forward, and as the teeth grow longer with time, it will be harder to reverse the crossbite. See the article One-sided Crossbite in Children for more information.

A frontal crossbite - SIDE CROSSBITE A crossbite involving the side primary molars means that the top jaw is smaller than it should be. In order for all the teeth to meet, and is an indication for immediate intervention.

A side crossbite in a 9 year old 
A side crossbite in a 8 year old - PREMATURE LOSS OF A PRIMARY MOLAR: If a baby molar is extracted due to an abscess or decay, and no provisions have been taken to keep the space open, teeth will drift towards the void, and no space will be left for the incoming permanent tooth.

A bonded space maintainer 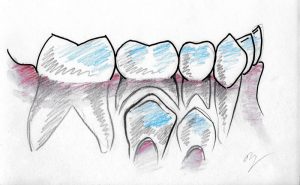
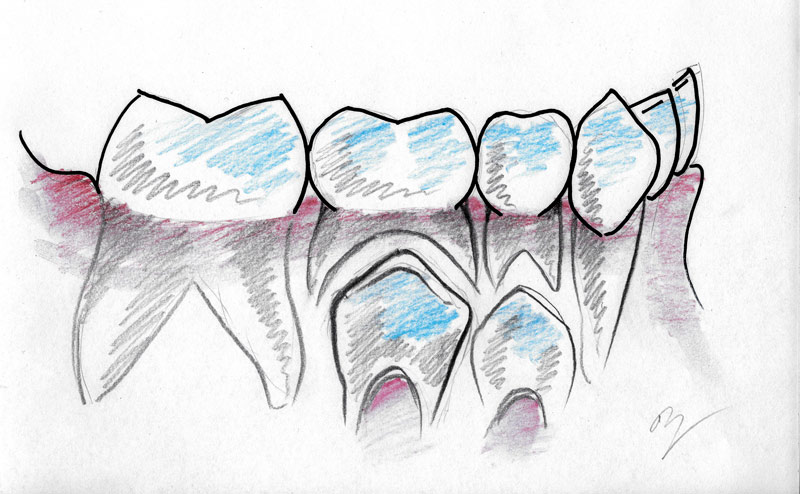
Illustration of baby molars 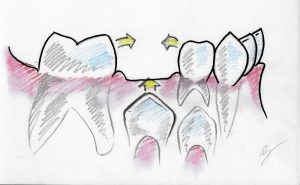
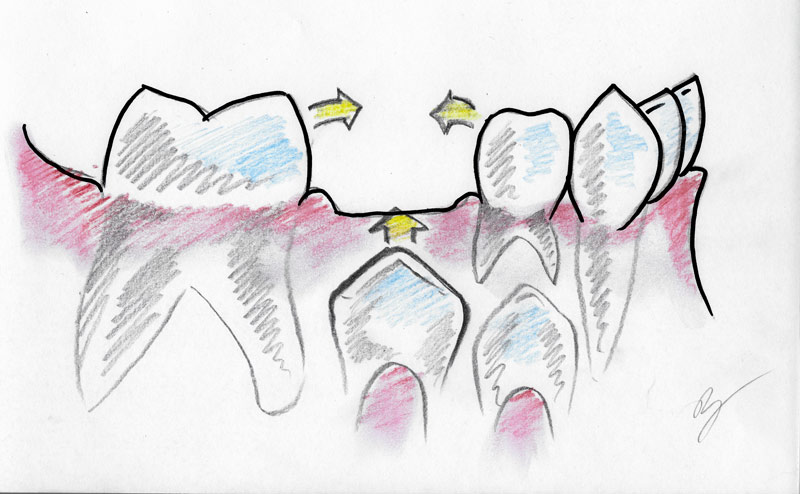
Illustration of baby molar extracted with no space maintainer 
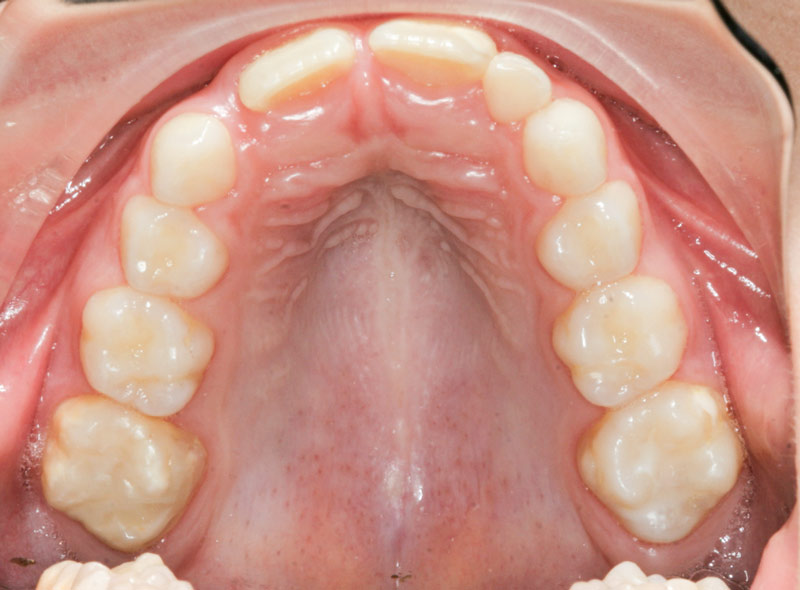
Illustration of permanent bicuspid being trapped - NO SPACE FOR LATERAL INCISORS: Around age 8, the permanent central incisor will erupt and take up a lot of space due to their size. Soon after, the upper baby lateral incisors fall, and if the arch size is insufficient, there will be very little space left for the permanent laterals to erupt. At this stage it is very evident that there will be crowding.

No space for lateral incisor - FLARED LATERAL INCISORS: If lateral incisors DO come in by age 9 when space is limited, they will come in rotated or flared sideways. This is a warning that there is going to be crowding. The underlying canines, due to lack of space on their eruption path are pushing against the roots of these laterals and shifting their position. As these canines come in a year later, they will find even less space. It is logical to deduce that crowding will NOT be outgrown, rather it will get worse. See also showcase Jaw Orthopedics in Children of Ages 7-10.

Rotated lateral incisors due to crowding 
Rotated lateral incisors due to crowding - DISPLACED CANINES: Around age 11 the upper canines will appear. Among all the permanent teeth, these ones travel the longest path before they emerge. They start their journey from the space right next to the nose, almost under the eye, and travel down over many years. If there is insufficient space, they will emerge “ectopically”, that is sideways, inside, or outside, or they will be impacted within the palate.

Crowded canines 
Crowded canines - PERSISTENCE OF BABY TEETH: If by age 12 one notices the “12-year” molars already erupted, the canines erupted, but the second primary molars still firmly in place, they have to be extracted. Otherwise the natural drift of the permanent teeth will not take place, and the lower canines will be crowded out.










SKELETAL SIGNS:
(these usually require a combination of early intervention jaw orthopedics and arch development)
- OVERCLOSED BITE: When a child bites down and the lower incisors are hardly visible, that means there is an overclosed bite, a vertical discrepancy, which has serious future consequences if not treated early. For more see the article Deep Bite And Orthopedic Bite Opening.

Overclosed bite - A GAP BETWEEN THE TOP AND BOTTOM INCISORS: If the front teeth do not meet when biting, there is a strong possibility that your child may be exhibiting a wrong swallowing pattern. A phenomenon that is termed “tongue thrust”, is usually the result of the tongue wedging between the front teeth every time the child swallows. This condition usually happens when the arch size is not large enough, but also propagates as the tongue develops a wrong “positioning” pattern which should be corrected by myofunctional therapy. See also the tongue thrust showcase Anterior Open Bite.

An open bite due to tongue thrust 
An open bite due to tongue thrust - BUCK-TEETH: protruding front teeth in 8-year olds is rarely the result of the upper teeth being too forward, but rather the lower jaw lagging behind. The flare of the upper teeth may, however, be exaggerated if the lower lip is constantly wedged between the upper and lower teeth.

Buck teeth




SIGNS OF CHILDHOOD SLEEP APNEA:
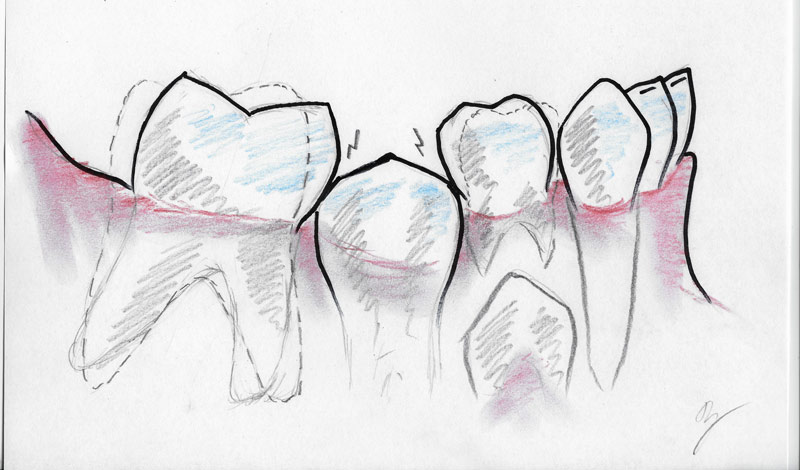
- WORN-DOWN INCISORS are a sure sign that the child has a grinding problem, or that the lower jaw wants to be positioned more forward, and is being held back by the small upper jaw. Nighttime grinding in children is a common sign of childhood sleep apnea.

Worn-down baby teeth - GRINDING of the teeth at night in children has been associated with an airway deficiency during sleep, mainly due to the lower jaw being retruded (further back), or a deep bite.

Worn-down baby teeth - SNORING at night is not normal in children and is usually the result of constricted airways due to adenoids, tonsils, and/or a retruded (underdeveloped) lower jaw.
- EARACHES and excessive earwax in a child have been attributed to the lower jaw being positioned too far back (retruded) and placing pressure on the jaw-joint and the ear.
- MOUTH BREATHING CHILDREN are susceptible to skeletal jaw anomalies. This may be due to chronic allergies, tonsil and adenoid enlargement, or other upper airway obstructions. It eventually forms a habit, the facial muscles lose their tone, and the mouth stays perpetually open. This causes a constricted upper arch with tooth crowding, a retruded lower jaw (that fails to grow forward), craniofacial deformities, dental crowding, and malocclusion. The far-reaching consequences are just so overwhelming, that dentists and orthodontists with a functional jaw orthopaedic approach, as well as speech therapists, should strive to address that issue and turn the child back to nose breathing before anything else. For more info, see the article Sleep Dentistry.


More on orthodontics principles – Jaw Facts…